The Friction Factor: Solving Delays in Clinical Trial Efficiency

Friction exists in every multi-stakeholder endeavor. Imagine the stakeholders in clinical trial design and implementation as a chain that links together participants lived experiences and biological responses into data that demonstrates outcomes. Multiple stakeholders from Pharmaceutical companies to patient panels, clinical research organizations (CROs) to technology vendors, interact as “links” to innovate better health outcomes for patients through better research outcomes.
The challenge is that each of these parties can be considered an added link in the chain of partners within the overall enterprise. For the trial to be successful, no link can break. But between every link, there is friction. This is the friction of all multi-stakeholder endeavors – each group has their own processes, jargon and assumptions may vary, and integrations may not be seamless. Thus, with every added link, the total friction within the system increases. This "friction" requires energy to overcome—the energy of time and/or money.
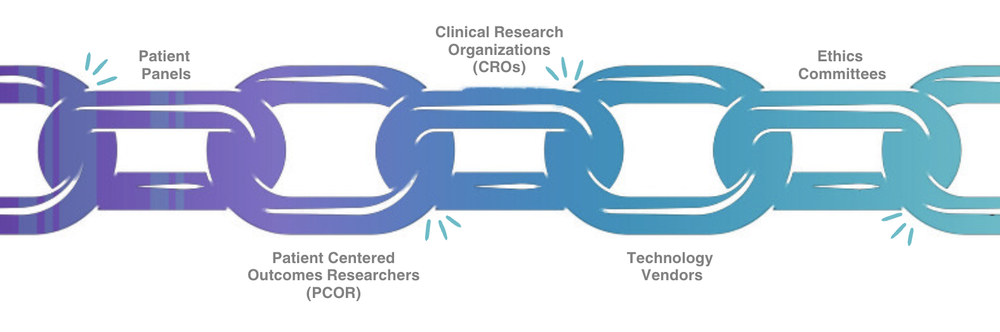
To compound these challenges, the links in the chain are growing. CROs deliver more services, technology providers have enhanced solutions, and researchers have more options for data collection than ever. The increase in solutions can be thought of as thicker chain links. The increased surface area means that there is even more friction between the links. While a limited analogy, this thinking partially explains why an individual organization adding enhanced services and solutions at times slows down a clinical trial. Yes, their link in the chain is "stronger", but the net "energy" required to deliver the study may be greater as a result.
This may seem like an impossible dilemma. If more links are needed and each link is becoming weightier, basic math argues that more time and money will be required to deliver studies with little hope of remediation in sight. One solution is to simplify clinical trials and remove links. In some rare cases, this is an option, but for many studies, this just isn’t a viable solution. This is where it is really important to follow our friction between two surfaces analogy: friction can be decreased. The question is - what decreases friction between the various stakeholders that make up the links in the chain of a clinical trial?
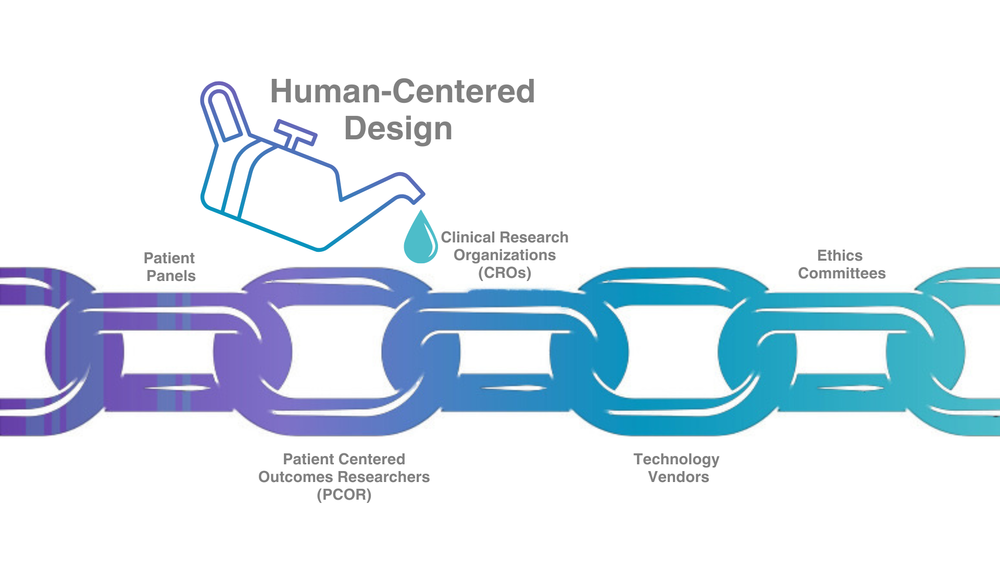
One of the key friction-decreasing "lubricants" for systems like trials are systems integrators. I don’t mean large (usually expensive) consulting organizations that provide these services. I mean practical solutions like Human-Centered Design (HCD) thinking applied to your study in a way that decreases the friction between components of the chain. HCD’s intersectional approach to design takes into account the practical needs of users and creates solutions by involving humans at every step. It’s a radically empathetic approach to the human beings who are engaged in the research, including PIs, clinical research site staff, data analysis teams, and most of all, the participants themselves. Ultimately, if applied correctly, an HCD approach can make a big difference in your study, no matter the stage of development.
There are four key principles to HCD as defined by the design theorist, Don Norman1 . Let’s take a minute to look at each one of these in light of a clinical trial being launched today to imagine how these principles could impact a study and decrease friction:
- People-Centered. What might your participants' lives be like? If you had the same condition, what do you imagine would make the schedule of assessments easier to follow? What if a home health provider came to you? What if some visits were fully remote? If you’re not sure what participants think, there are accessible and rapid methods using modern technology to ask potential participants.
- Understand and solve the right problem. This comes up all the time in conversations about technology and regulators. Obviously, ethical and data integrity considerations are top priorities. However, I often see conversations devolve into asking "what’s easiest to explain," which is often answered "what we’ve always done," instead of asking "what is the best solution, and how do we effectively communicate the value of that solution to key parties?"
- Everything is a system. Each piece of a clinical trial is a system within a system. The medical, regulatory, and telecommunications systems, as well as the internal cultures of each company, are nexuses of human interaction that push and pull on each other in visible and invisible ways. One approach I’ve found that can be really unifying across systems is to visually map out the journey of participants, sites, vendors, and data throughout a study to understand where each of the systems are interacting and identify potential high-friction nodes where extra solution-thinking might be required.
- Small, simple interventions. Trial complexity is not decreasing, but small changes can make a big difference. Start with selecting the right endpoints, organize with the experience of participants in mind, map out the study journey, and when possible, select data collection platforms that are built on HCD principles.
An HCD approach won’t solve all the challenges in clinical trials. It won’t decrease complexity, make the links smaller, or cut back on the number of links needed to deploy a study. But, in my experience, when properly applied, the HCD principles of being people-centered, understanding and solving the right problem, thinking in systems, and coming up with small, simple interventions can dramatically decrease the friction that exists across the system. And remember, friction represents time and money.
I believe HCD can make a real impact by decreasing friction within clinical trials. But there are other means of decreasing friction. One is to develop cross-functional understanding between scientists and operators. More on that next time...